Ryan,
As you mentioned, there seems to be a consensus that there are two kinds of deep stops.
During the UHMS Deep Stops workshop in June, there were two types of deep stops defined. There was a lot of discussion about how to define them, but my understanding was this:
Empirical Deep Stops
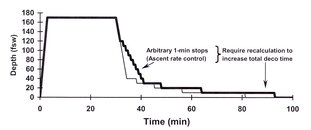
Stops that are added to the decompression stops derived from the model. Some examples would be Pyle stops, microbubble stops, or GF stops. I see these as stops that are in addition to the basic stops. These deep stops extend the total decompression time. This is shown in the first graph.
Model-derived Deep Stops
Stops that are an inherent part of the model. Some examples would be RGBM, VPM, and VVAL-18. These plans tend to show a shortened overall decompression time with deeper initial stops.
One of the primary studies presented was one done by NEDU.
As I understand it, the deep stop profile was derived from a Navy bubble model. But it was modified to create dives that would have symptoms. If you have no incidents, you have no data points. By the way, that is one of the reasons that this is important data. The end-point was injured divers, not high bubble scores. There are not many places in the world you can do this kind of research. I don't think it would be legal in Canada any more. We owe these guys.
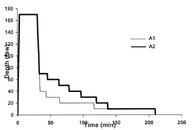
The experimental dives are shown in the second graph.
To put this in perspective, the scientists involved expected to show that deeper stops would improve the outcome or at least be "not worse." That was not the result.
While this isn't proof that deep stops don't work, it isn't promising either. There are a few caveats though.
1. This tested profiles where the overall dive time was the same as without the deep stops. Typical bubble models create this sort of profile with deeper stops and the same or shorter total profiles.
This doesn't say anything about deep stops that extend the decompression like Pyle stops, microbubble stops, or GF stops.
2. This was an air test. Maybe trimix dives would have different outcomes.
3. This tested specific profiles. Maybe different profiles would have had different outcomes.
In addition, there were other studies presented and discussed. The best that could be said is that the evidence for deep stops was conflicting.
I am not a doctor or physiologist. The room was full of those guys and if I am getting this wrong, I invite corrections.
Bruce
The attached graphs are Copyright C 2008 Undersea and Hyperbaric Medical Society Inc.



")

