
Scubagolf
Contributor
Deleted.
Last edited:


Welcome to ScubaBoard, the world's largest scuba diving community. Registration is not required to read the forums, but we encourage you to join. Joining has its benefits and enables you to participate in the discussions.
Benefits of registering include
Swimming horizontally under water is not the same as a vertical ascent, especially with a good tissue load of nitrogen as would likely be the case when running out of air in a deep dive. I think there is a high risk of injury running out of air on a deep dive.Now, I also agree that we should avoid OOA situations. But my feeling is that with sufficient watersmanship (or waterswomanship) OOA by itself should not induce panic. It can easily be coped with in normal sport diving environments (defined is less that 120 feet depth, with no "overhead" environments, including no decompression obligations).
SeaRat
---------- Post added February 17th, 2013 at 07:20 PM ----------
I am curious as to why this thread was moved from the Accidents and Incidents forum to the Basic Scuba forum?
John
I was very careful to define this as "sport diving" which by definition does not have high tissue loads of nitrogen. Sport diving to me is no-decompression diving, and no "overhead environment" (ice, cave, wreck) diving. I actually said that in the quote, but I will repeat it here too. So you are right in that respect, this does not apply to deep diving.Swimming horizontally under water is not the same as a vertical ascent, especially with a good tissue load of nitrogen as would likely be the case when running out of air in a deep dive. I think there is a high risk of injury running out of air on a deep dive.
Rich, I have worked in professional safety for over 35 years now, and the DAN accident sequence is unique to DAN. That is the trigger (Initiating root cause), harmful action (root cause as an effect of the trigger), disabling injury (causes death or makes drowning likely), and cause of death (COD) specified by the coroner. This is probable unique because DAN was limited by the types of information available to them about the scuba fatalities.I agree, for me the first rule of diving is "If you panic you die". The other thing I believe is that a lot of times it is a couple of seemingly unrelated problems happening at the same time that can cause a serious problem. Most divers understand and train for the big problems but a couple of small problems that many may not train for happening together can cause confusion followed by panic.
---------- Post added February 17th, 2013 at 11:13 AM ----------
Was there any breakdown of what type of dives they were doing?
For diving, I would like to concentrate on the decision-making box. I am trying to promote decision-making that gives the diver options. Many times, factors come together that overwhelm the person trying to make the decision. By having more options, there are better choice selections available to the diver. What I'm trying to get away from is what I feel is a pre-disposing factor--saying that if you run out of air, you will die. As I have shown, that doesn't have to be the case. If we pre-dispose divers to think that there is no alternative but the buddy, an alternative air source, and they do not have those available, panic like you described is more likely.I'll write about that later.
I was very careful to define this as "sport diving" which by definition does not have high tissue loads of nitrogen. Sport diving to me is no-decompression diving, and no "overhead environment" (ice, cave, wreck) diving. I actually said that in the quote, but I will repeat it here too. So you are right in that respect, this does not apply to deep diving.
I'll explain later the reasons behind the way I was able to swim 75 feet after not having air today.
SeaRat
---------- Post added February 17th, 2013 at 11:58 PM ----------
Rich, I have worked in professional safety for over 35 years now, and the DAN accident sequence is unique to DAN. That is the trigger (Initiating root cause), harmful action (root cause as an effect of the trigger), disabling injury (causes death or makes drowning likely), and cause of death (COD) specified by the coroner. This is probable unique because DAN was limited by the types of information available to them about the scuba fatalities.
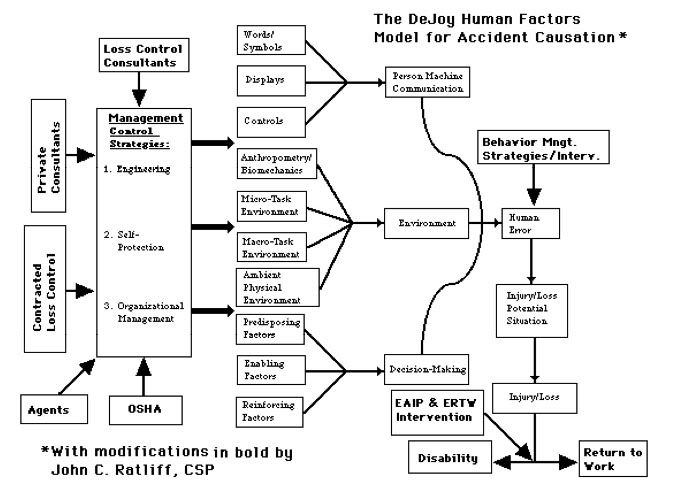
There are other models that I have used over the years. Dan Peterson talks about overloads, mismatches and traps which cause errors. I have used fault tree analysis to isolate the factors which come together in an accident. And I have used David DeJoy's Human Factors Model of Accident Causation. That model looks like this:
Note that all these factors cause a human error which leads to the accident, injury/fatality.
For diving, I would like to concentrate on the decision-making box. I am trying to promote decision-making that gives the diver options. Many times, factors come together that overwhelm the person trying to make the decision. By having more options, there are better choice selections available to the diver. What I'm trying to get away from is what I feel is a pre-disposing factor--saying that if you run out of air, you will die. As I have shown, that doesn't have to be the case. If we pre-dispose divers to think that there is no alternative but the buddy, an alternative air source, and they do not have those available, panic like you described is more likely.I'll write about that later.
SeaRat
Was there any breakdown of what type of dives they were doing?
I was very careful to define this as "sport diving" which by definition does not have high tissue loads of nitrogen.
I come from an earlier time. We ran out of air many times in my early diving (1959-67). But we were taught differently. When I finally got certified by LA County in 1963, our pool harassment session consisted of the instructor putting a gill net over us, and having us untangle ourselves. In the process he would turn our air off, and we'd take a breath and nothing was there; buddy breathing under the net was necessary to pass his course (LeRoy French was the instructor's name). Our equipment was different too, with the J-valve and no SPG being used. At times the J-valve would accidentally be bumped and we would not have that 300 psi remaining as it had already been pulled. This was fairly normal.
I have been thinking about your position for a while. Although I agree with the concept that if people are competant and fit, that they should be able to swim up in a "low on air" emergency. However,,, a big HOWEVER dive training now is so short, that it is entirely impractical to try to develop the skills and instil the level of confidence that you (and I) think is essential for safe diving. In the current dive training environment... teaching people to NOT run out of air is probably a much better use of time, then spending a few moments telling them they CAN swim to the surface.
If dive training prgrams really wanted to instill this level of confidence and proficiency, they would require some freediving ability.. even to a depth of 25 or 30 feet... but that is past the capabilities of probably many scuba instructors....
I know when I taught my young sons to scuba dive, they were required to be able to freedive. But it just ain't gonna happen in today's training environment.
[video=youtube;IyLYmEMoKE4]http://www.youtube.com/watch?v=IyLYmEMoKE4&feature=share&list=UU1utDku8vJ RJYgBZImLyLJQ[/video]
Ken, what I was speaking to was a sport diver as I knew him/her. In the 1970s through 1980s, we used to teach people not to get close to the "knife edge" of the no-decompression tables. Now, apparently people are becoming dependent upon their dive computers to tell them where they are concerning nitrogen loading. So I agree that in this age, it may be easy to get into a decompression situation unknowingly. I also know from reading some of the threads that there is concern about non-consistency in the alarms that these computers put out. I was in the pool a few weeks ago with two other divers, who were testing their gear for a subsequent vacation. There was a LP leak in a BC secondary regulator that they needed to attend to. But the computer, apparently sensing this leak, was beeping about air consumption that was "too fast" according to the divers. The idea with these computers is that they have now become the "go to" device rather than a backup to dive planning. In doing so, we may be sacrificing the ability to surface directly--without decompression.Not to split hairs here John, but I don't think "high" needs to mean "deco." You can be at 99% of the predicted nitrogen load and still be within sport diving (no-deco) limits. And there are plenty of instances of divers who either do a rapid ascent to change the equation and make a no-deco dive into a missed-deco dive, or instances where - due to body physiology - the tables or computers (theoretical mathematical models) don't apply to that particular person. So while that table/computer may be saying "not bent," the body is saying "Get me to a chamber!!!"John C. Ratliff:I was very careful to define this as "sport diving" which by definition does not have high tissue loads of nitrogen.
...Expiration, normally passive, results from the elastic recoil of the lungs when thoractic expansion ceases. The increasing intra-thoractic pressure then forces the gases from the lungs into the atmosphere.
From a functional point of view, the lungs can be subdivided into:
1. Total lung capacity (TLC): the lung content when lungs are inflated from total collapse to maximum inflation.
2. Vital capacity (VC): the amount of air which can be inhaled after maximal expiration.
3. Residual volume (RV): amount of air remaining in the lungs after maximal expiration: volume from maximum expiration to collapse.
4. Inspiratory capacity (IC): amount of air which can be inhaled after normal expiration.
5. Functional reserve capacity (FRC): amount of air remaining after normal expiration.
6. Inspiratory reserve volume (IRV): amount of air which can be inhaled beyond normal inhalation.
7. Tidal volume (TV): amount of air inhaled and exhaled in a normal breath.
8. Expiratory reserve volume: amount of air which can be exhaled after normal expiration.
The accompanying chart shows the relative size of these components. In diving, the divisions of chief interest are the tidal volume, residual volume, and total lung capacity.
Residual volume is about 20 per cent of total lung capacity in young males and rises with age. Recall that the ratio of residual volume to total lung capacity determines the depth where lung squeeze will develop. [Note: now disproven--there is a blood shift which keeps lung squeeze from occurring in deep breath-hold dives. jcr] With a high ratio, RV small in comparison to TLC, more compression of lung volume can occure before RV is reached...
") I was at 18 feet depth. In fresh water, 2 atmospheres absolute pressure is at 34 feet. That means that from 34 feet, a volume of air going to the surface will expand to twice its volume. 18 feet divided by 34 feet equals 0.53. So if I divide my 1.5 liters by 0.53, I get 2.83 liters of air available in my lungs for my surfacing from 18 feet depth. This is why, even with having exhaled to my residual volume at 18 feet, once I started climbing "up" toward the real surface, I was able to exhale.
I was at 18 feet depth. In fresh water, 2 atmospheres absolute pressure is at 34 feet. That means that from 34 feet, a volume of air going to the surface will expand to twice its volume. 18 feet divided by 34 feet equals 0.53. So if I divide my 1.5 liters by 0.53, I get 2.83 liters of air available in my lungs for my surfacing from 18 feet depth. This is why, even with having exhaled to my residual volume at 18 feet, once I started climbing "up" toward the real surface, I was able to exhale.
