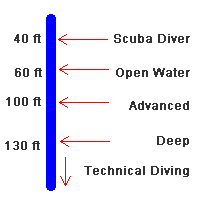
It is spelled out pretty clearly, but you do have to read the material. 60 ft is the recommendation for new divers, and the mandatory limit for an OW class. Deeper than that (to change the recommendation) needs experience and/or training. Thus AOW provides a 100 ft recommendation, Deep Specialty allows diving to full certification depth, i.e. 130 ft.
PADI does not recommend 30 ft/min. It says to not exceed 60 ft/min, or to follow what your computer says, whichever is slower. All modern computers are slower...typically 30 ft/min.
Nope. You are still taught rescue breaths, which are NOT optional for drowning. You should probably re-certify for your CPR....it's due every two years.
Depth recommendation-- I'm probably splitting hairs. I know it says needs experience and/or training. If you don't get the needed training, I don't think exactly what amount of experience you need is spelled out.
Ascent rate--Yes, you are right of course. I read into this as implying that PADI leans more toward all (or most of) the other agencies recommendation of 30'. Again, if you don't use a computer, I don't think the possible "slower" is spelled out. Perhaps the advent of most folks using computers nowadays is the reason for this wording. I assume most computers will beep if you exceed 30' per minute, but I am no expert.
Don't get me wrong--I'm not at all saying PADI is at fault for not spelling out these picky details. These are things that you should do logically--such as not " well, I dived to 70' last week, now I have experience so I'll next go to 100". I'm just saying they are not spelled out.
Rescue Breaths-- This has been discussed on SB maybe a year or so ago, not sure exactly. Maybe the standards for EFR or other CPR courses have changed yet again and I am wrong. A detailed description that non- medical pros were to do only chest compressions and no rescue breaths was presented by someone. Again, I or this person's data could be wrong. No requirement for me to take CPR a 5th time as I am not an active DM anymore. I believe that the 2 year requirement when I was was a shop requirement. It may have been and still may be PADI's standard that active instructors & DMs must CPR recertify every 2 years--there was no need for me to know this because I had to anyway due to shop policy. I don't know the legalities of performing CPR holding an expired card.
I will not take CPR again--I review my manual a bit every day and to be honest, can't be bothered to know what the latest changes may be. This has changed several times since 2009.
Regarding to still being taught rescue breaths regarding drowning are you possibly referring to in the PADI Rescue Course? In the 2 times I took CPR with St.John Ambulance (Canada) there was never any reference to drowning and water. This course is much more thorough than EFR. My 2 times taking EFR were before they removed (?) recsue breaths for non medical people.