Not read the whole thread, but I had a PFO which I found by getting bent.
Potentially relevant though is that I dived on and off for years (5-37) with no clinical DCS, a few times I was tired, but this was '75-97 so a lot of air and not much nitrox until post 94.
I trained and qualified as a DM in the UK, and used an Oceanic computer for what we now call recreational diving. It was very conservative if you followed it's traffic light system.
Around 95 though I got involved in tech and started doing longer, deeper, planned deco, lots of deep air and some trimix.
Mostly I was fine, but I did pick up skin bends and finally some neuros (visual disturbance).
However on reflection I am fairly sure that the bends correlated with post dive exertion, either a spine ladder in twins and stage, ladder from boat to dock carrying gear, or hauling tech rigs up hills at quarries.
Ergo it's the physical exertion that pushed the crap through the hole.
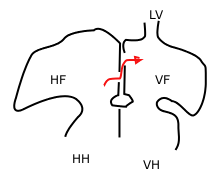
At my PFO diagnosis, even a Valsalva would shove the champagne into the wrong place.
So, my point is that it's possibly less the wet profile and more the post dive profile that finds the holes.