This basic description is OK from a generalized wide angle point of view. But once the specific of the dive situation is added, some extra description is needed. The above described the on gassing, but missed the off gassing side of the equation during the dive and surface.
"Tissues that are at a lower tension will continue uptake until they reach saturation or the pressure is reduce below their tension pressure.
In ascent, this also applies in the opposite direction. Tissues on/off gas towards the inspired pressure line, which is always less than the divers ambient pressure. Hence while holding a stop, any tissue that is faster than the current ceiling limiting one, will be off gassing. A tissue that drops its pressure below the ambient line, contributes no further stress to the dive. This occurs in all dive profile patterns - shallow and deep. Any tissue that on gassed from the deeper stop, but also has a faster time than the current limiting one, will no longer have any influence on the ascent.
"If you have two dives of equal length where one moves to shallower depth faster, it will have less saturation than the one which holds a deep stops"
Whilst true, it is a hypothetical situation. Real dive models all get longer for the same dive and deeper stops, because of internal gas tracking changes. All models have this ability built in now.
But, this extra on gas, may not change the actual decompression limit or required time by any significant amount. A deco model sets it limits based on the maximum value of any one discrete cell limit values. If during the course of the dive, no significant change in cell pressure is observed,
at the time that cell becomes limiting then deco times may change only slightly.
In the case of deep vs shallow stops the difference in gas load is actually quite minor. The cells have been subjected to typically 30 mins of full depth (7?) ATA differences. When it comes to the ascent, and the different in stop types, the extra pressure changes are small in the tissue, when compared to the depth exposure just carried out. i.e deep stop add very little extra to the overall gas volume.
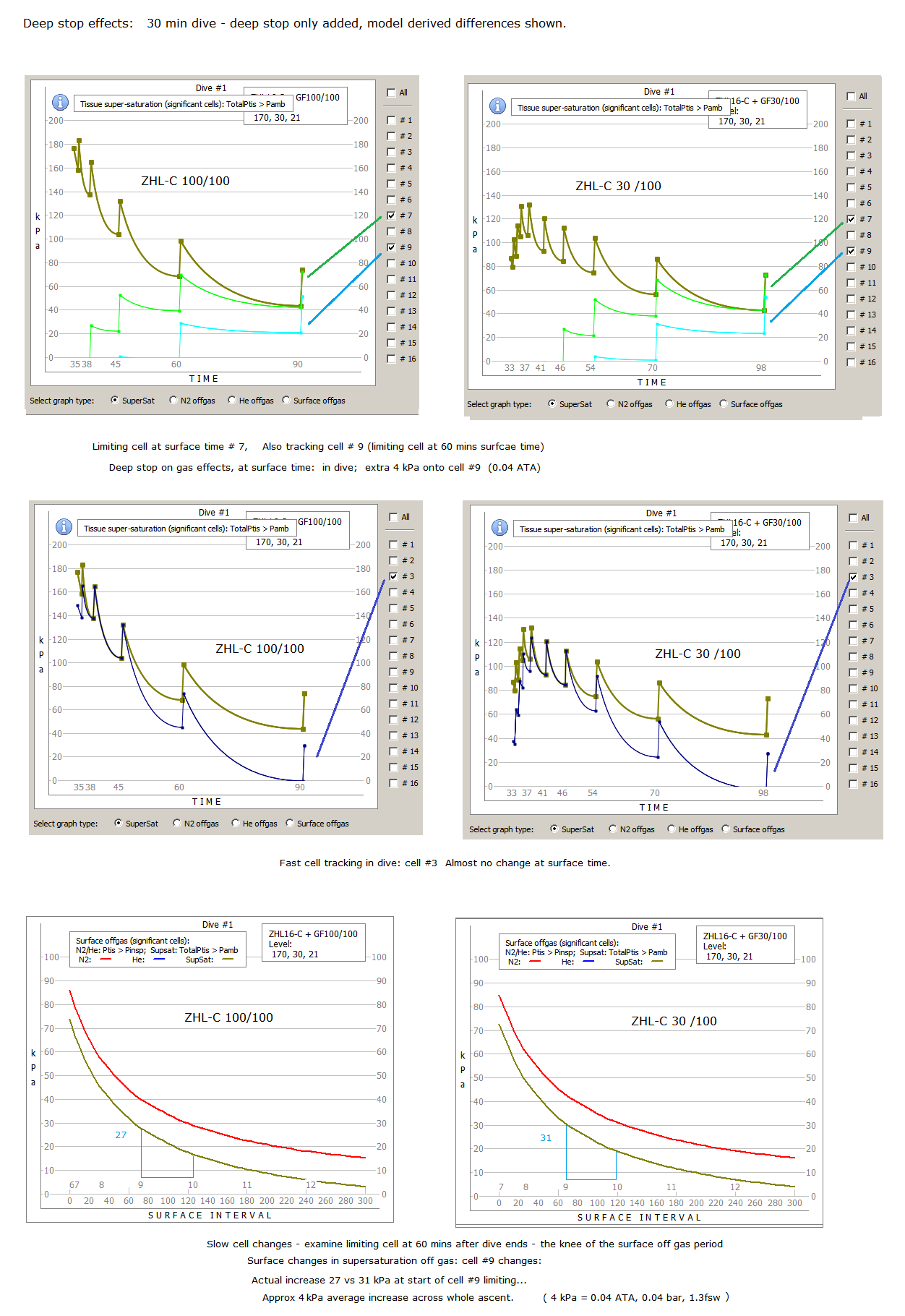
This graph compares two profiles: with / without deep stops, and examines the resulting stress changes.
It hard to see much difference at all. That's because the deep stop changes are tiny compared to the effects of the bottom time segment. In this sample, it adds about 12% to the deco time.
You can see in the pure deep stop comparison:
- Fast cells have half the decompression stress in the deep stop dive.
- Fast cell time surface pressure not affected by deep stops.
- The most affected slow cell in deep stop (#9), at surface time, only rose 4kPa .
- The surface stress / off gas has risen by an average of 4kPa across whole ascent.
The real world affect of a deep stop approach, is to significantly decrease in-dive stresses, but only increase surface stress and required deco time by a small amount.
.



")

