For an unbiased look and review of VGE and it role in DCS, readers might like to see this paper:
Venous gas embolism as a predictive tool for improving CNS decompression safety
This is by a research group with many years of work, studies and papers in the topic of VGE.
As they say in the paper,
"This illustrates that having detectable bubbles yields only a 4% chance of developing DCS. Even when using high bubble grades as test criterion, the positive predictive value is low..."
***********
The simple reality: Fast deco has high supersaturation tissue pressure (decompression) stress, fast offgas rates, and it excites VGE into higher growth. BUT... the reverse implied connection is wrong. High VGE does not imply high decompression stress, because high VGE can / do occur even when only lower decompression stress exists. The correlation is not 1:1.
All divers give different VGE scores. You and me can do the same dive together - and we will have different VGE scores - everytime. Some divers make no VGE (0), and some divers make a lot of VGE and bubble like a well shaken bottle of coca-cola. Trying to force all divers to conform to a size 2, is futile.
Do not confuse tissue DCS and VGE ! VGE is not tissue bubbles.
VGE does not predict DCS.
Do not confuse Bubble models with VGE ! Bubble models work with tissue micro-bubble growth - not VGE.
Normal tissue DCS is theorized to grow from "extra vascular" bubble growth. This is your standard everyday DCS risk, and its what all deco models try to control and regulate - tissue bubbles - type 2 DCS. Controlling a dive by means of supersaturation stress levels, is the most accurate and reliable prediction / avoidance tool we have.
David Doolette:
"Supersaturation is a required condition for bubble formation and growth. There is broad (universal?) agreement that modelling tissue gas uptake with a range of exchange rates - as we do for instance with a collection of compartments with mono-exponential gas exchange - captures the essential processes,..." ref
*****
The VGE bubble is "intra vascular" (grows in the veins). It grows from gas that has most probably already left the tissue, and is gas that is probably in transit to be exhaled by the lung. They are not tissue bubbles.
VGE does not normally cause us DCS - its usually filtered out in the lung, or dissolves quickly in the arterial side... except.... VGE will cause Pulmonary DCS - if you ascend directly to the surface, or do commercial / mil style surface chamber deco. VGE also has some connection to PFO / pulmonary shunt induced DCS - see DAN report.
****
The DAN PFO workshop report describes issues of PFO / shunts and gives good summary suggestions.
However, one aspect of a PFO / shunt has been overlooked.... A PFO recirculates blood - unfiltered blood, that still contains high levels of inert gas. This will lead to an effective increase in inspired inert pressure, and as a result, we probably do not off gas as fast as planned.
Therefore, a good question might be: is a PFO induced DCS caused by rouge arterialized bubbles clogging up the plumbing? Or by higher tissue pressures than is planned? Or ?
*********
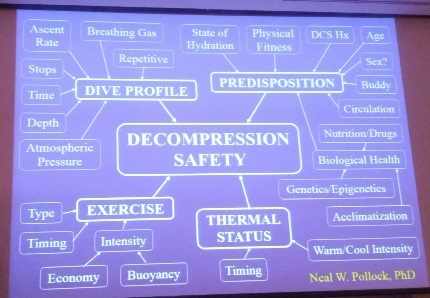
Here is the summary slide from the Dr. Neal Pollock presentation on Decompression Stress at the TekUSA 2016.
Note the salient points: VGE does not equal DCS. It can be a relative, but NOT an absolute indicator of stress, and needs to be used cautiously.



")

