UWSojourner
Contributor
Of course you like it.... it's a one sided nonsense measure, that always favors the shallow profile..... junk science... which is why you let Kevin make it up and use it.... so you can avoid being blamed for it later on.
.
See this post (or just go back 6 posts) as your comment was already addressed.
....
Integral supersaturation is not that difficult. Supersaturation is necessary for bubble formation. More bubbles are formed with higher supersaturation pressures. More bubbles are formed with longer supersaturation exposures.
Integral superaturation just sums up (supersaturation exposure) x (time your exposed) for the entire dive and surface period until supersaturation is no longer present.
It's just an index of decompression stress for dives of the same run time.
....
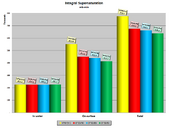
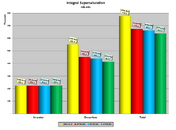
For example, a CCR 270ft 20min 10/70 1.2 1.6@20ft dive produces the following index of decompression stress for 4 different profiles -- VPM-B+2, GF20/90, GF30/88, GF50/82 (all dives have the same run time):
You can see that the profile recommended by VPM-B produces the most decompression stress. As Dr. Pollock stated, this is simply a loading problem. The diver diving VPM-B+2 incurs about 25% more deco stress at the surface than does a GF30/88 diver.
You can see why VPM-B might incur more deco stress exposure if you look at the peak GF chart below. The fact that VPM-B "sags" below the other profiles during the deeper portion of the dive is an indication of its recommended deep stops. Those deep stops delay effective off-gassing and continue on-gassing in intermediate and slow tissues.
Hope that helps.