I suspect that is EXACTLY the hazarded 'guess' - an extrapolation of results not substantiated by the trial design.
Hello,
Your points about the hazards extrapolating the results of studies beyond the study parameters are, of course, well made and accurate. However, in this case the extrapolation is not quite in the realms of guesswork. It sounds as though you have read the original technical report. If not, please (I was going to say pm me and I will send it....
But I see you have read it.
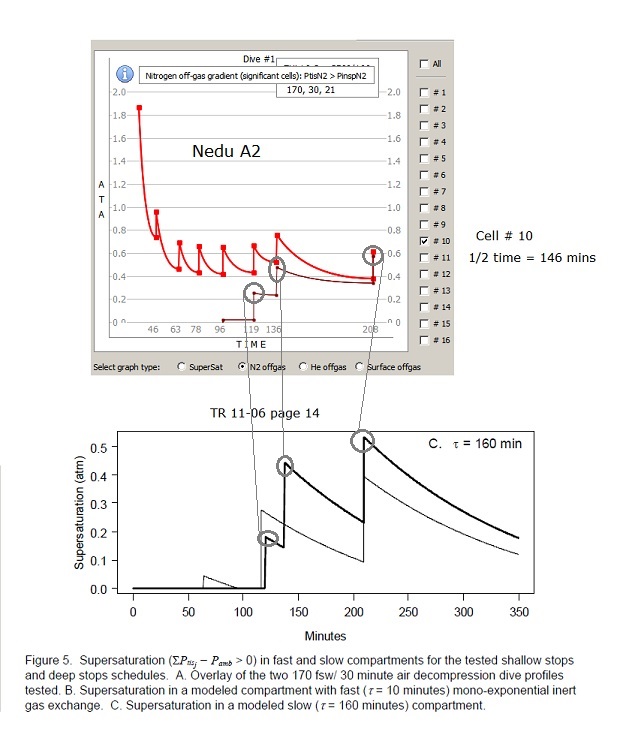
So, you will have seen that there was quite a lot of thought given to the reasons for the result which was somewhat unexpected. There is quite a long section in the report dealing with the analysis of supersaturation patterns in fast and slow tissues, and analysis of the deep stops skew (similar to the integral supersaturation evaluations that have been discussed here). All of this is related to the heat map evaluations that uwsojourner has produced.
On the basis of these analyses, which applied well established physiological principles in both decompression physiology and decompression sickness pathophysiology, an extremely plausible (indeed, possibly the only plausible) explanation for the result was derived. The extrapolation that is occurring here is an extrapolation of that principled analysis to the broader range of deep stop decompressions (hence the comparisons of supersaturation patterns between VPM and GF undertaken by uwsojourner). The fact that the apparently detrimental patterns of supersaturation that almost certainly explained the result in the NEDU study can also be seen in the profiles that emphasise deep stops when compared to profiles with less emphasis on deep stops suggests that outcomes for the former would likely be worse than the latter. It is clearly not proof, but it is the best evidence we currently have to base our "opinions" on. And never lose sight of the fact that there is NO EVIDENCE whatsoever pointing in the other direction.
Simon M
Last edited:
")