
Yep, Google the "Accessory Muscles of Respiration"Hello,
Diaphragmatic movement is not the only avenue for lung expansion. Upward and outward movement of the chest wall would also accommodate lung expansion.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Confused on AGE; holding breath OK if lungs are near-empty?
- Thread starter ScubaSamScubaStevesFather
- Start date
-
- Tags
- age barotrauma
Please register or login

Welcome to ScubaBoard, the world's largest scuba diving community. Registration is not required to read the forums, but we encourage you to join. Joining has its benefits and enables you to participate in the discussions.
Benefits of registering include
- Ability to post and comment on topics and discussions.
- A Free photo gallery to share your dive photos with the world.
- You can make this box go away
Gelirfella
Contributor
. In general we try to keep airway pressures less than 30 cmH2O and the threshold for a significant risk of pulmonary barotrauma in healthy lungs is probably around twice that (which can be generated with an ascent from about a meter underwater if the lungs are full at the start of the ascent).
Sure, but I’ve personally seen multiple pneumos in intubated patients. Everyone watches the peak and plateau pressures in the unit and in the OR but sometimes it happens. In the aggregate probably more frequently than pneumothorax from dive injuries I would suspect. I’ll look into what the incidence of pneumothorax is from PPV but I’d wager it’s higher than the incidence of pneumothorax from diving and yet I have never heard of an air embolism from PPV. Not to say it hasn’t happened.
It should be added that these patients are sick and their lung compliance is not the same as that of healthy lungs for the most part. Divers do have healthy lungs so therein may lie a significant difference.
johndiver999
Contributor
I can't answer all your questions, but I have ascended rapidly a few times and forgot to exhale. What I experienced in these situations was a feeling of excess and uncomfortable expansion of the lungs, which was enough of a reminder to me to exhale immediately, which I did. I did not suffer any noticeable trauma from these incidents.That’s a fair point. I’m not sure if the physiology of breath hold diving applies perfectly. are there any cases of air embolism documented from a short duration dive? Also, it is an incredibly rare event though pneumothorax is more common. Why would it not be more common than it is? Perhaps, the circumstances that lead to direct pressurization of gas into the arterial system are just extremely rare. Or perhaps it requires a person with specific microbubble formation characteristics, depth, time, and ascent profiles? Free divers that can achieve those depths may already have been selected to be individuals with decreased susceptibility? I didn’t make this theory up as I’ve said. I just find it to be more plausible than the alternative.
One incident was playing around in very shallow water and jumping off the bottom (extremely stupid) and he other was a rescue situation where I became hyper-focused on the victim and literally forgot to breathe and fell back into free diving instincts ( I guess).
I think that if your lungs are healthy, you probably really have to lock your glottis down (from a spasm or panic response) in order to get hurt - as the chairman has said, "keep your airway open and you should be fine" is my paraphrase of his comment. These are the reasons why I think lung over expansion injuries are not so frequent.
Hawaiianbrian
Registered
Lets see. You have a little air in your lungs, you're holding your breath, you're making a rapid ascent because you are out of air and going to use CESA because you are deep. Pulmonary barotrauma and AGE are the least of your worries.A chest CT scan can reveal physical obstructions caused by disease etc. Obviously not a practial solution for a person who seems healthy, but something to consider for a diver with any signs of lung disease. A slight persistant cough or feeling out of breath from moderate physical activity could be warning of underlying lung issue that could cause problems for a diver.
This sums up a first hand experience with pulmonary barotramua and AGE. Despite following the rule of constant breathing, air trapping on ascent occured in a very localized area of the lungs. In this case the physical defect was caused by minor bronchiectasis that was not discovered until after the accident.
But you don't hold your breath if you do a CESA, unless you want to have an AGE. No point in getting to the surface if you embolize.Lets see. You have a little air in your lungs, you're holding your breath, you're making a rapid ascent because you are out of air and going to use CESA because you are deep. Pulmonary barotrauma and AGE are the least of your worries.
dmaziuk
Contributor
Lets see. You have a little air in your lungs, you're holding your breath, you're making a rapid ascent because you are out of air and going to use CESA because you are deep. Pulmonary barotrauma and AGE are the least of your worries.
They can fix bent. What they can't fix is stupid. And also: dead.
Good point. On top of underlying lung pathology/poor compliance, the mechanism of injury is different - repeated pressurization and depressurization with high (but still within "safe" limits) inspiratory pressures against a stiff or inflamed lung vs. a single event in a healthy diver that involves higher pressures than those seen in any ventilated patient.Sure, but I’ve personally seen multiple pneumos in intubated patients. Everyone watches the peak and plateau pressures in the unit and in the OR but sometimes it happens. In the aggregate probably more frequently than pneumothorax from dive injuries I would suspect. I’ll look into what the incidence of pneumothorax is from PPV but I’d wager it’s higher than the incidence of pneumothorax from diving and yet I have never heard of an air embolism from PPV. Not to say it hasn’t happened.
It should be added that these patients are sick and their lung compliance is not the same as that of healthy lungs for the most part. Divers do have healthy lungs so therein may lie a significant difference.
Best regards,
DDM
Next

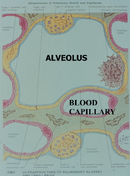
I think you meant cell layers. Last I heard, animals don't have cell walls. Critters I work with do!Yes, you’re missing something; that something is that there is only two cell walls thickness between the capillaries and the alveoli.
Seaweed Doc, yes, you are correct. I just found a my files from my M.S.P.H. degree studies, and one by Douglas A. Swift, M.D., M.S.P.H., a PowerPoint presentation titled "Occupational Pulmonary Disease," contained this slide picture of the alveolus and blood capillary interface which further explains what I was trying to get across. There is little between the interior of the capillary and the inside of the arterial capillary. I have made the edit here, as I could not do it in the original post (time to edit had apparently past). Thanks for the correction.John C. Ratliff:
Yes, you’re missing something; that something is that there is only two cellwallslayers thickness between the capillaries and the alveoli.
Next
I think you meant cell layers. Last I heard, animals don't have cell layers.Critters I work with do!
SeaRat
Attachments
Next
I think you meant cell layers. Last I heard, animals don't have cell walls. Critters I work with do!
umm.....cell layers or cell membrane layers?....precision begs the question.
-Z
Similar threads
- Replies
- 11
- Views
- 1,035
- Replies
- 15
- Views
- 1,576
- Replies
- 1
- Views
- 1,157
- Replies
- 7
- Views
- 1,638
