
My pleasure. Glad we could help.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Returning to diving after an Perilymph Fistula
- Thread starter accurist
- Start date
Please register or login

Welcome to ScubaBoard, the world's largest scuba diving community. Registration is not required to read the forums, but we encourage you to join. Joining has its benefits and enables you to participate in the discussions.
Benefits of registering include
- Ability to post and comment on topics and discussions.
- A Free photo gallery to share your dive photos with the world.
- You can make this box go away
Dr. Mike and DDM, your information has been very helpful to me and is greatly appreciated. I'll let you know how I get on. Thank you for your time.
Regards,
Dan
No problem, always happy to help, and thanks for understanding the limits of what we can do here. But please feel free to keep us posted, especially after you see the otologist. These threads are often useful years later in the archives when people share their experiences...
Good luck!
Mike
These threads are often useful years later in the archives when people share their experiences...
One thing I would like to add at this stage to anyone reading this thread, is to be very careful when performing an Valsalva manoeuvre.
I'm no expert, but from what I understand there are safer techniques for clearing the ears, that are worth taking the time to master.
P.S. DAN have been amazing throughout my whole episode, can't say enough good things about them.
One thing I would like to add at this stage to anyone reading this thread, is to be very careful when performing an Valsalva manoeuvre.
I'm no expert, but from what I understand there are safer techniques for clearing the ears, that are worth taking the time to master.
P.S. DAN have been amazing throughout my whole episode, can't say enough good things about them.
Accurist,
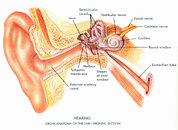
Thanks for adding that. More specifically, divers should be careful when performing the Valsalva maneuver if they're having difficulty equalizing. The excerpt below is from an article we recently wrote for the DiveAssure online newsletter. It may be helpful to reference the attached diagram of the middle ear when reading it.
"If a diver attempts to force a Valsalva maneuver, the air may enter the middle ear all at once and overpressurize it. The extra pressure in the ear makes the tympanic membrane suddenly bow outward. The ossicular chain then pulls on the oval window and makes it bow outward as well.
The oval window is part of the inner ear. The organs of the inner ear, the cochlea and semicircular canals, are filled with fluid and are responsible for hearing and balance, respectively. The round window is located inferior to (below) the oval window. It acts like a damper for the pressure waves that are transmitted to the inner ear via the ossicular chain and oval window. When the oval window presses inward, the round window bows outward, and vice versa. This mechanism allows the pressure of the fluid in the inner ear to remain relatively stable as the ossicular chain vibrates in response to sound waves. However, if the oval window is suddenly yanked outward because of a forceful Valsalva maneuver as explained above, the round window may be drawn inward so much that it tears. This is known as a perilymph fistula, and it is considered a medical emergency. Symptoms of a perilymph fistula can include hearing loss, ringing in the ear, vertigo, nausea, and vomiting. If not treated promptly, it may result in permanent damage to the middle ear."
Attachments
One thing I would like to add at this stage to anyone reading this thread, is to be very careful when performing an Valsalva manoeuvre.
I'm no expert, but from what I understand there are safer techniques for clearing the ears, that are worth taking the time to master.
Absolutely, as DDM has pointed out in the last post, a forceful Valsalva can under certain conditions cause middle and even inner ear damage! The Toynbee maneuver is a good gentle alternative (swallowing with the nose closed).
P.S. DAN have been amazing throughout my whole episode, can't say enough good things about them.
+10 to that, I won't dive without a DAN insurance card...!
When it first happened I went to lay down in a cabin because of the nausea and vertigo. I remember feeling like the left side of my face was numb, not sure if it was because I was laying on my face or if it was caused by the PLF. The numb feeling cleared up quickly, probably within an hour. In the above diagram I see the 'facial' nerve is close to the inner ear, could the nerve have been temporary effected?
When it first happened I went to lay down in a cabin because of the nausea and vertigo. I remember feeling like the left side of my face was numb, not sure if it was because I was laying on my face or if it was caused by the PLF. The numb feeling cleared up quickly, probably within an hour. In the above diagram I see the 'facial' nerve is close to the inner ear, could the nerve have been temporary effected?
The facial nerve is almost entirely a motor nerve (it moves the face muscles). There is a very small area of the face (mainly in the ear canal) in which sensation is carried by the facial nerve, but that would probably not be the cause of any of the numbness that you described...
... The numb feeling cleared up quickly, probably within an hour. ...
The trigeminal nerve is largely responsible for facial sensation.
"Quickly" and "hour" used together sounds a bit off to me. Pressure-induced numbness tends to resolve in minutes after normal circulation is restored; sometimes with pain and tingling. If it happens again, I suggest having it checked; medications, injury, infection are considerations. OTOH, abrupt, sudden unexpected numbness or weakness must be treated as an emergency.
Does prompt repair of the round window after the injury alter your recommendation regard discontinuing diving? I developed brief tinnitus and hearing loss on ascent from a 70' dive 20 years ago. My ENT diagnosed PLF and repaired my round window. My hearing loss has been stable since and the vertigo only lasted seconds at the time of injury. I sat out for years, but a few years ago rolled the dice and got back in the water.
Does prompt repair of the round window after the injury alter your recommendation regard discontinuing diving? I developed brief tinnitus and hearing loss on ascent from a 70' dive 20 years ago. My ENT diagnosed PLF and repaired my round window. My hearing loss has been stable since and the vertigo only lasted seconds at the time of injury. I sat out for years, but a few years ago rolled the dice and got back in the water.
Unlike repair of the tympanic membrane (eardrum), which follows a fairly standard course, PLF recovery and recurrence is much less understood and less predictable.
Remember, I am not specifically recommending any plan of action - I really can't do that over the Internet. But I wouldn't conclude that a more rapid surgical repair would preclude a recurrence of the PLF.
It is, as you correctly pointed out, a roll of the dice!
")
Dive safe,
Mike
Similar threads
- Replies
- 2
- Views
- 228
- Replies
- 9
- Views
- 1,130
- Replies
- 7
- Views
- 534
