Barotrauma: The Ins and Outs of the Pops and Cracks
By Eric Hexdall, RN, ACHRN @Duke Dive Medicine
Article courtesy DiveAssure, originally published on Medical Articles – DiveAssure
Many of us know the feeling. We’re on descent and realize that one of our ears hasn’t equalized. We perform the Valsalva maneuver, and SQUEAK! The air zips in, we may feel some momentary pain, and the pressure in the ear goes away. We continue the dive, perhaps with the ear gurgling and snapping, and surface with the most common injury in diving: middle ear barotrauma.
Boyle’s Law states that as pressure around an air-filled space increases, the volume will decrease proportionally, and vice versa. In practice, this means that all of the air-filled spaces in and around our bodies can be affected in one way or another by pressure. When we dive, these spaces need to be equalized as the pressure around us changes.
The sinuses are filled with air as are, of course, our lungs. Air trapped beneath faulty dental work can cause extreme discomfort, and gastrointestinal air can be an issue for some of us. Our diving gear can also create air-filled spaces. Our masks trap air against our faces, and if we use a dry suit, there is an air-filled space between the suit and our bodies.
Typically, barotrauma of descent is called a "squeeze" or "block", and barotrauma of ascent is called a "reverse squeeze" or "reverse block". The air-filled spaces in and around our bodies may be affected by one or both of these. We’ll examine each of them.
Ear Barotrauma
There are several areas in the ear that are vulnerable to barotrauma. Before we discuss them, let’s take a closer look at the anatomy of the ear.
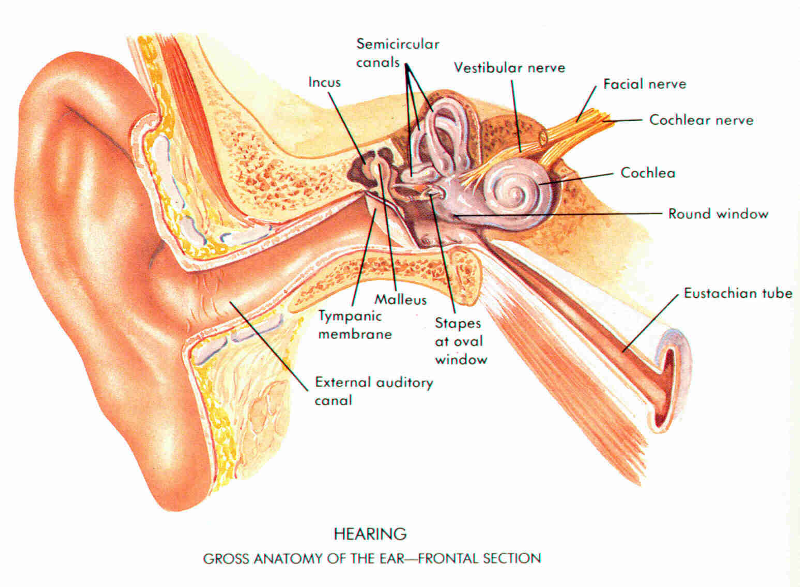
The middle ear, located just behind the tympanic membrane, contains the three bones of the ossicular chain: malleus, incus, and stapes. It is filled with air and is equalized via the Eustachian tube, which connects the middle ear to the nasopharynx (the area of the throat just behind the nose). In young children, the Eustachian tube travels through flesh and mucous membrane and is oriented more horizontally. Because of this, their ears do not drain or equalize as easily as an adult’s. This can cause them to experience discomfort with relatively small pressure changes and makes them more vulnerable to middle ear infections.
As we get older, the end of the Eustachian tube that is closest to the middle ear (called the distal end) becomes encased in bone and so becomes less prone to collapse. As the head grows, the orientation of the Eustachian tube changes so that fluids drain more easily from the middle ear. The end of the tube that is closest to the nasopharynx (the proximal end) remains soft and travels through flesh, which is why it is more difficult to equalize the ears on descent than on ascent. If a diver gets behind on equalizing, the proximal end of the Eustachian tube may collapse and make it difficult to clear the ear without ascending first. If the diver continues without equalizing, the air inside the middle ear will follow Boyle’s Law and reduce itself in volume.
Several things can occur at this point. The tympanic membrane begins to bow inward and may rupture if the diver continues descending. Also, blood and/or serous fluid can be pulled from the delicate capillaries that line the middle ear. This fluid fills the middle ear and may even relieve some of the pain and/or pressure that the diver is experiencing.
If a diver attempts to force a Valsalva maneuver, the air may enter the middle ear all at once and over-pressurize it. The extra pressure in the ear makes the tympanic membrane suddenly bow outward. The ossicular chain then pulls on the oval window and makes it bow outward as well.
The oval window is part of the inner ear. The organs of the inner ear, the cochlea and semicircular canals, are filled with fluid and are responsible for hearing and balance, respectively. The round window is located inferior to (below) the oval window. It acts like a damper for the pressure waves that are transmitted to the inner ear via the ossicular chain and oval window. When the oval window presses inward, the round window bows outward, and vice versa. This mechanism allows the pressure of the fluid in the inner ear to remain relatively stable as the ossicular chain vibrates in response to sound waves. However, if the oval window is suddenly yanked outward because of a forceful Valsalva maneuver as explained above, the round window may be drawn inward so much that it tears. This is known as a perilymph fistula, and it is considered a medical emergency. Symptoms of a perilymph fistula can include hearing loss, ringing in the ear, vertigo, nausea, and vomiting. If not treated promptly, it can result in permanent damage to the middle ear.
A diver with a suspected perilymph fistula should stop diving immediately and be transported to the nearest emergency department as soon as possible. Keep the diver’s head up, and caution him to avoid straining or attempting to clear his ears, both of which can aggravate the condition. Obtain a careful dive history, including previous dives and time of onset of the symptoms. Perilymph fistula can mimic inner ear decompression sickness, so a good history will help the treating physician make the correct diagnosis. Even after treatment, a diver with perilymph fistula may have residual symptoms such as high-frequency hearing loss and/or tinnitus.
Rarely, air can become trapped in the middle ear and fail to vent on ascent. If one ear clears before the other, a diver may feel alternobaric vertigo related to the differing pressures on the semicircular canals. It can be frightening and disorienting, especially if it happens in the water. If a diver experiences alternobaric vertigo, it is helpful to grab onto something stable until it passes. To reorient herself, a diver can observe her bubbles. Once the ear clears, the vertigo should abate. In rare cases, reverse middle ear squeeze can result in outward rupture of the tympanic membrane or perilymph fistula as described above. A diver who feels symptoms of reverse middle ear squeeze should slow his or her ascent and attempt to equalize the ears by swallowing. The Valsalva maneuver should be avoided, as this can increase the pressure in the middle ear and cause injury.
A tightly fitting hood may cause air to become trapped in the external ear canal. If this occurs, the air between the hood and the tympanic membrane will be compressed on descent. A diver may interpret this as a need to add more air to the middle ear space. However, adding air to a middle ear that is already equalized under these conditions may result in injury to the tympanic membrane and/or inner ear. Hoods should be snug but not excessively tight. It may be beneficial to pull the hood away from the face before descent to allow water to enter the external ear.
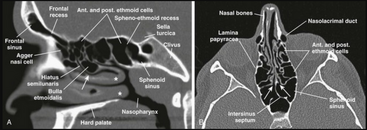
Sinus Barotrauma
The ear and sinuses are related in that they are both affected by colds, allergies, and other irritants. The sinuses are cavernous spaces in the skull that serve to warm, humidify, and filter incoming air. There are four sets of sinuses, shown below: frontal, maxillary, ethmoidal, and sphenoidal.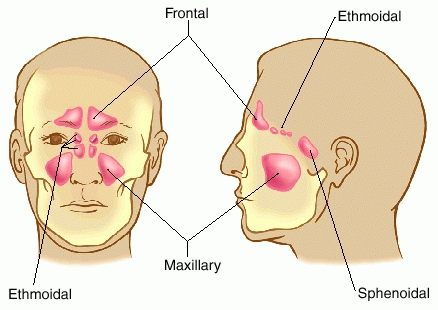
If a diver begins a descent with blocked sinus openings, the air in the affected sinus will be compressed. This exerts a pulling force on the mucous membranes, and can result in rupture of the tiny capillaries and subsequent entry of blood into the sinus. This is usually a relatively painless occurrence, so the diver often remains unaware of what is happening. On ascent, as the remaining air in the sinus expands, the blood and mucus may be expelled into the mask or drain down the nasopharynx and into the mouth. As ominous as it may appear, sinus squeeze is usually a relatively benign occurrence and heals with rest and avoidance of pressure changes.
On the other hand, the opening to the sinus may become so irritated as to not allow air to escape on ascent. This results in reverse sinus squeeze, which may be painful enough to prevent a diver from further ascent. This can become problematic in SCUBA as the diver’s gas supply is depleted. A diver with reverse sinus squeeze should continue to slowly attempt to surface. In the author’s experience, temporarily assuming a head-down position can direct fluid away from the openings of the sinuses and allow them to equalize.
Proper ear equalization techniques, moderation of the descent rate, and avoidance of diving while congested are all strategies that can help keep a diver’s ears and sinuses healthy and happy. But, what if you’re on that dream liveaboard vacation? You’ve saved for two years, spent thousands of dollars, flown halfway around the world and now you’re stuffed up because the hacking fellow in the seat next to you was overly generous with his germs. All may not be lost; there are a few strategies that can help get you in the water.
- Decongestants. Over-the-counter decongestants like pseudoephedrine (Sudafed, others) can be helpful. Over-the-counter antihistamines like diphenhydramine (Bendadryl, others) and loratadine (Claritin, others) can be beneficial if the congestion is due to allergies. Many of these medications may cause drowsiness, so use them with caution and do not dive if you experience sleepiness or sedation. Always follow all dosing instructions, and beware of medication interactions, especially with prescription drugs. Consult your physician if you have any questions about your medications.
- Non-steroidal anti-inflammatory medications (NSAIDs). NSAIDs like ibuprofen (Motrin, others) can help reduce the inflammation and swelling of the mucous membranes. Again, follow dosing instructions, beware of medication interactions, and consult your physician if you’re unsure about medications.
- Sinus rinses and saline nasal spray. Several over-the-counter sinus rinses are available. They typically come with pre-mixed packets of salt and sodium bicarbonate to make an isotonic (compatible with body electrolytes and pH) liquid that will not irritate your sinuses. Saline nasal sprays are gentle enough to use frequently and can help keep secretions clear.
- Go slowly. Don’t try to push it on your descents and ascents. When equalizing, stay ahead of the descent. That is, actively equalize your ears even though it doesn’t feel like you have to. Try different equalization methods to see which works best for you. On ascent, do not add any air to your middle ear. Go slowly enough to allow your ears to equalize themselves.
- Do not dive if you’re unable to equalize. If you’ve tried all of this and you’re still unable to clear, do not dive. Serious injury can result, and evacuation from remote areas can be difficult.
Lung Squeeze and Pulmonary barotrauma
Lung squeeze of descent is not typically encountered in compressed gas diving. However, free divers may suffer from lung squeeze if the lungs are compressed beyond their residual volume, or the amount of gas that remains in the lungs after a full expiration. Typically, residual volume in an adult is about 1 liter. If the same typical adult took as deep a breath as possible, the total volume of the lungs would be about 5 liters. If we work a little Boyle’s Law math on these numbers, we can predict the depth at which the lungs will be compressed to their residual volume: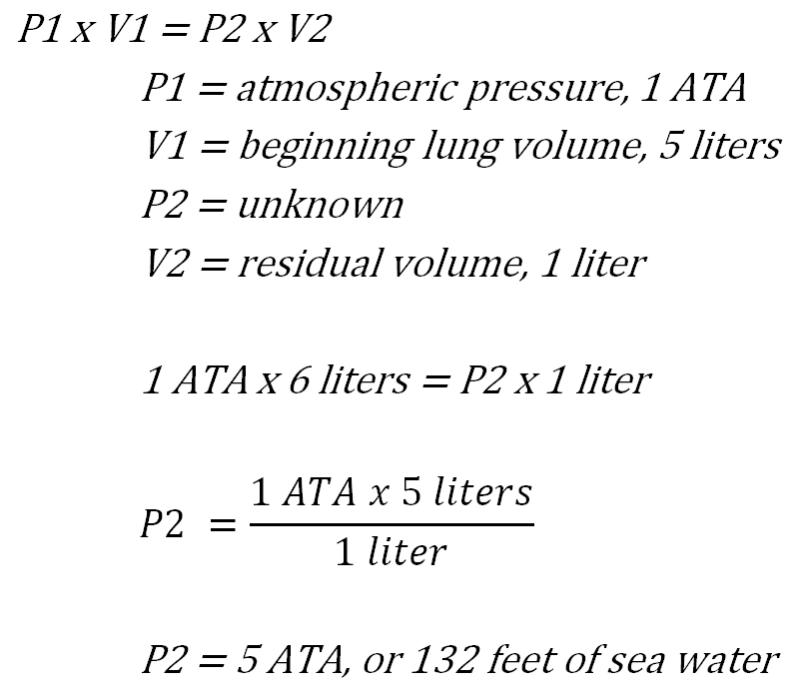
So, theoretically, beyond a depth of 132 feet, an average person would be at risk of lung squeeze during a free dive. However, free divers who can attain a depth of 132 feet and greater probably would not be described as "average". As of this writing, the current unlimited freediving depth record is held by Austrian Herbert Nitsch, who plunged to an astounding depth of 253.2 meters (830.8 feet of sea water, or 26.17 atmospheres absolute) in June 2012 (source: www.herbertnitsch.com). At that depth, his lungs were compressed to about 4% of their original volume. So, why don’t competitive free divers like Herbert suffer from fatal lung squeeze? In brief, the immersion-related shift of blood into the organs of the chest cavity (sometimes up to a liter or more) protects the chest itself from trauma. Also, trained free divers use a variety of techniques and exercises designed to maximize lung capacity and minimize potential damage to the lungs when they descend beyond the theoretical maximum (Ferrigno and Lundgren 2003). The emphasis is on the word "trained". Formal instruction is highly recommended for those wanting to explore this area of diving.
Reverse lung squeeze is better known as pulmonary overinflation. As all divers learn, holding the breath on ascent can result in rupture of the delicate alveoli and capillaries in the lungs. This may lead to pneumothorax (air between the lungs and chest cavity), mediastinal emphysema (air in the space between the lungs and around the heart), subcutaneous emphysema (air beneath the skin), and/or arterial gas embolism. Air can also be trapped by bullae (air-filled cysts in the lungs) or by restricted air passages related to reactive airway diseases like asthma.
Pulmonary overinflation is a medical emergency. Divers with suspected pulmonary overinflation should be placed on oxygen by qualified personnel and monitored carefully for breathing and circulation, then evacuated to the nearest emergency department by the quickest means possible. Prevention strategies include awareness of breathing, diving within one’s own limits, and screening of dive candidates for physical conditions that may predispose them to air trapping.
Gastrointestinal barotrauma
Since the gut is designed to contract in order to move food along the digestive tract, air trapped in the gut that is compressed on descent will not affect a diver. However, the reverse is not true. Expanding air in the gut on ascent can cause distention and pain. If a diver feels gastric distention on ascent, the ascent should be halted and an attempt made to expel the offending gas. The U.S. Navy Diving Manual addresses this in a frank and succinct manner: "The diver should… attempt to gently burp or release the gas anally. Overzealous attempts to belch should be avoided as they may result in swallowing more air." (NAVSEA 2016). Gastric distention on ascent can normally be prevented by avoiding foods known to produce gas, especially if the diver is particularly prone to such problems.Tooth barotrauma
Also known as barodontalgia, tooth barotrauma can be an extremely painful occurrence. Air may be trapped under a filling due to decay or improper placement. In a diver, this air will be compressed on descent. This can exert a pulling force on the pulp of the tooth, resulting in pain.If a filling is not properly sealed, it may become pressurized at depth. When the diver ascends, the air will expand and may crack the tooth or expel the filling.
Prevention of barodontalgia involves ensuring that fillings are free of air. Dentists typically do not leave air beneath fillings, but it is advisable for a diver to inform his or her dentist that he or she dives, and ask for extra caution in placing a filling. If a diver experiences barodontalgia on descent, the dive should be immediately aborted. If barodontalgia occurs on ascent, the diver should ascend as slowly as possible given his or her decompression status and remaining gas supply. This will best facilitate air venting around the filling and thus possibly allow the diver to avoid cracking the tooth or expelling the filling.
Face mask squeeze
Mask squeeze results from failure to add air to the mask via the nose on descent. The air in the mask will be compressed and may cause the delicate capillaries around the eyes to rupture. This can result in reddening of the sclera and ecchymosis (bruising) around the eyes, along with swelling of the eyelids and conjunctiva (lining of the eyelid). Surprisingly, the diver often does not feel pain when this happens. The results are dramatic but are normally relatively benign and should resolve in a couple of weeks. Pain or changes in vision should be addressed immediately in the nearest emergency room. Face mask squeeze can be prevented by adding air to the mask on descent. On ascent, the air in the mask will simply expand and either enter the diver’s respiratory system or vent itself through the seal.
Face mask squeeze. Image courtesy Lester Quayle and Rita Barton.
Suit squeeze
Since they trap air, dry suits also present an opportunity for barotrauma. As the air in the suit is compressed on descent, folds of skin may be trapped in the creases on the suit. This is easily prevented by gradually adding air to the suit on descent.
Dry suit squeeze. Image courtesy Oakville Divers.
On ascent, a dry suit diver needs to vent air from the suit to prevent overinflation and blowup, or uncontrolled ascent. While not technically barotrauma, a blowup can result in decompression illness or pulmonary overinflation.
Whole Body Squeeze
There are case reports of surface-supplied hard-hat divers suffering from severe, sometimes fatal barotrauma when their gas supply umbilical was suddenly depressurized, either by severing the umbilical at the surface or through mechanical failure (e.g. thread failure on a topside air fitting). If there is not a working check valve attached to the diving helmet, the air in the helmet (and attached suit, if the diver is in a fully enclosed dry diving dress) will rush up the umbilical due to the pressure difference between atmospheric pressure and the pressure on the bottom. Since the gas supply umbilical is flexible but rigid, the effect of this is to produce a large negative pressure in the umbilical, which acts like a powerful vacuum. If the diver is deep enough, diver’s body may be literally sucked into the helmet.To avoid this, part of the safety checklist for military and commercial diving involves testing the check valve for functionality prior to attaching the helmet to the umbilical.
The laws of physics can’t be circumvented, only compensated for. Barotrauma is much better prevented than treated, and by applying your knowledge of Boyle’s Law along with appropriate diving training, you can avoid squeeze.
References
Ferrigno, M. and C. E. Lundgren (2003). Breath-Hold Diving. Bennett and Elliott's Physiology and Medicine of Diving. A. O. Brubakk and T. S. Neuman, Elsevier Science: 153-180.NAVSEA. US Navy Diving Manual, Revision 7A, 2018